Number 70, August 2011
Lara J. Akinbami, M.D.; Xiang Liu, M.Sc.; Patricia N. Pastor, Ph.D.; and Cynthia A. Reuben, M.A.
Data from the National Health Interview Survey, 1998–2009
Attention deficit hyperactivity disorder (ADHD) is one of the most common mental health disorders of childhood (1). The symptoms of ADHD (inattention, impulsive behavior, and hyperactivity) begin in childhood and often persist into adulthood. These symptoms frequently lead to functional impairment in academic, family, and social settings (2,3). The causes and risk factors for ADHD are unknown, but genetic factors likely play a role (4). Diagnosis of ADHD involves several steps, including a medical exam; a checklist for rating ADHD symptoms based on reports from parents, teachers, and sometimes the child; and an evaluation for coexisting conditions (5). Recent national surveys have documented an increase in the prevalence of ADHD during the past decade (6,7). This report presents recent trends in prevalence and differences between population subgroups of children aged 5–17 years.
Keywords: race, ethnicity, poverty status, National Health Interview Survey
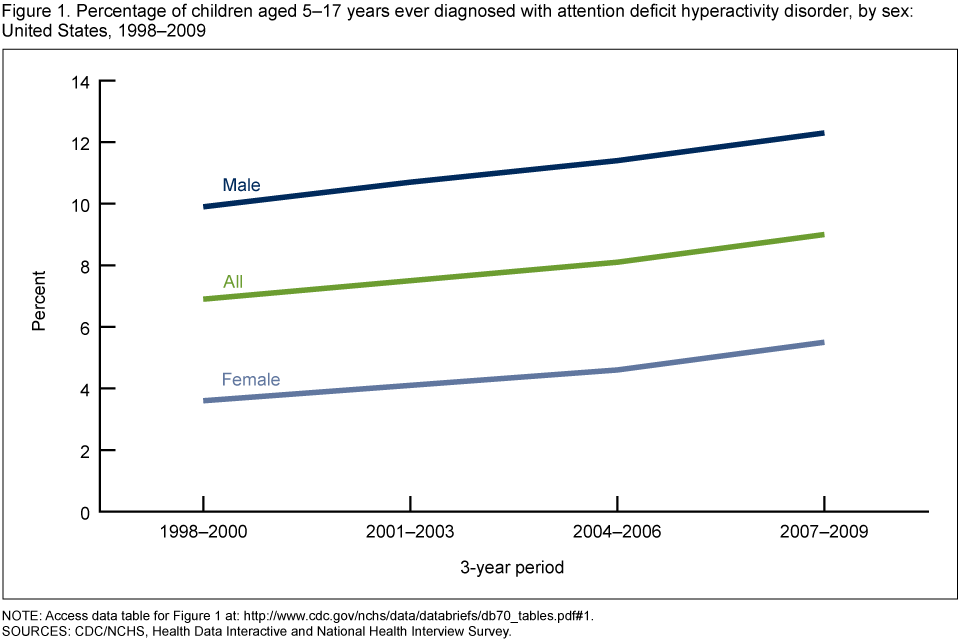
NOTE: Access data table for Figure 1Â
SOURCES: CDC/NCHS, Health Data Interactive and National Health Interview Survey.
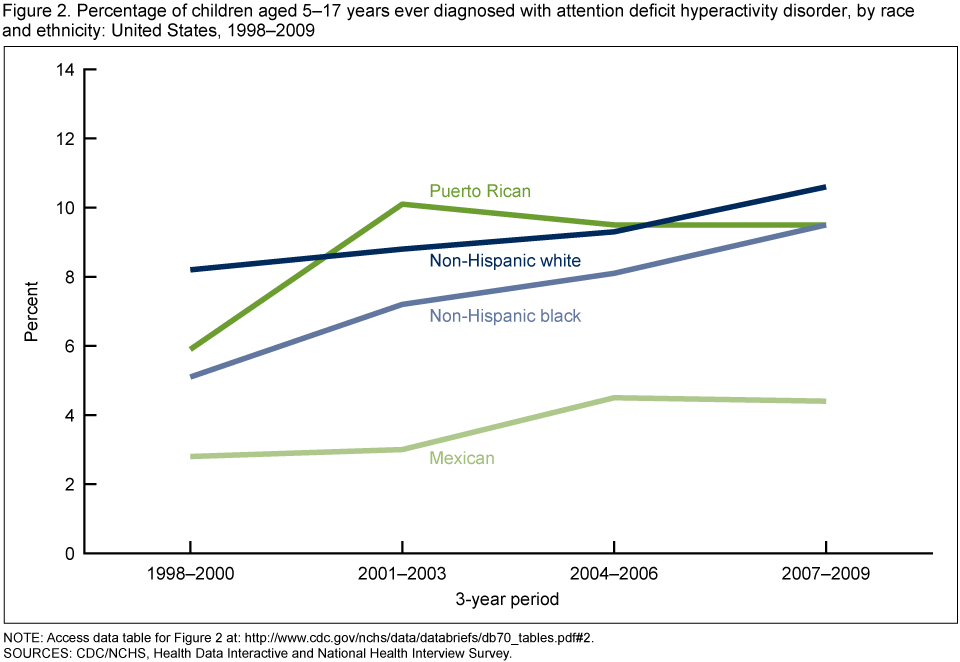
NOTE: Access data table for Figure 2Â
SOURCES: CDC/NCHS, Health Data Interactive and National Health Interview Survey.
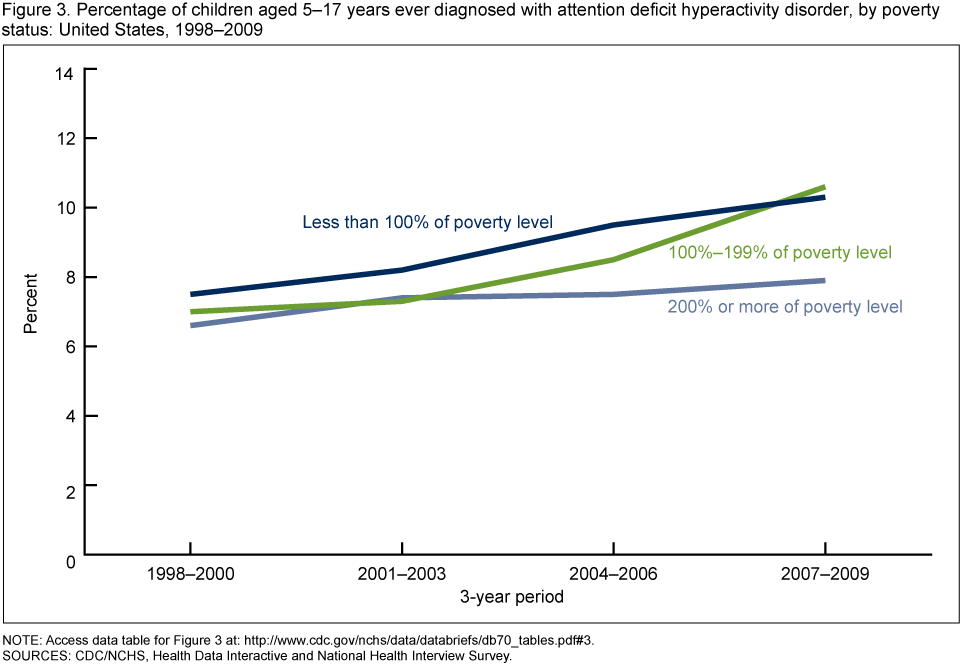
NOTE: Access data table for Figure 3Â
SOURCES: CDC/NCHS, Health Data Interactive and National Health Interview Survey.
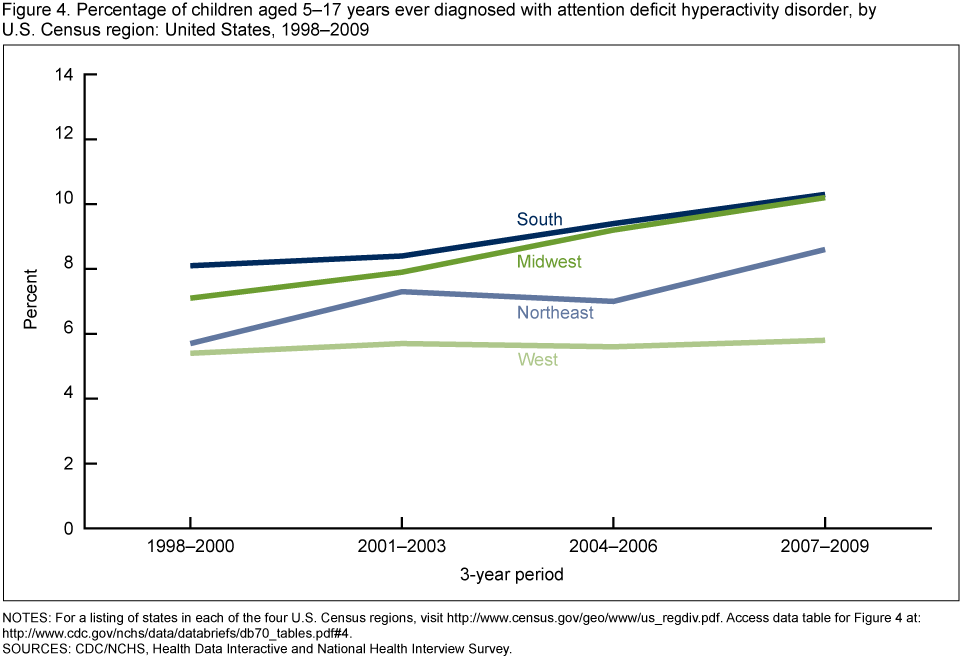
NOTES: Access data table for Figure 4Â
SOURCES: CDC/NCHS, Health Data Interactive and National Health Interview Survey.
From 1998–2000 through 2007–2009, the prevalence of ADHD increased among children aged 5–17 years, from 6.9% to 9.0%. These increases were seen among both boys and girls, among children in most racial and ethnic groups except Mexican children, and among children with family income less than 200% of the poverty level. By geographic region, ADHD was more prevalent in the South and Midwest regions of the United States than in the Northeast and West regions during 2007–2009. Prevalence estimates in this report are based on parental report of the child ever receiving a diagnosis, and thus may be affected by the accuracy of parental memory (including recall bias), by differential access to health care between groups (diagnostic bias), or by willingness to report an ADHD diagnosis. One study that included clinical assessment of children for ADHD symptoms (8) found that only one-half of children meeting the criteria for ADHD had received a diagnosis of ADHD or regular medication treatment. For the present report, it was not possible to discern whether growing prevalence indicates a true change in prevalence or increased detection and diagnosis of ADHD. Nevertheless, the societal costs of ADHD—including those associated with medical, educational, and criminal justice resources—are large (8).
ADHD prevalence: Estimated based on the number of adults responding “yes” to the question, “Has a doctor or health professional ever told you that your child had Attention Deficit Hyperactivity Disorder (ADHD) or Attention Deficit Disorder (ADD)?” This question is included in the standard National Health Interview Survey (NHIS) Sample Child questionnaire.
Poverty status or percentage of poverty level: Based on family income, family size, the number of children in the family, and, for families with two or fewer adults, on the age of the adults in the family. The poverty level is based on a set of income thresholds that vary by family size and composition. Families or individuals with income below their appropriate thresholds are classified as below the poverty level. These thresholds are updated annually by the U.S. Census Bureau to reflect changes in the Consumer Price Index for all urban consumers (9). Estimates by poverty status from NHIS are based on both reported and imputed family income (10).
All ADHD prevalence estimates were obtained from the Health Data Interactive (HDI) table, “Attention deficit hyperactivity disorder, learning disability, behavior difficulty, ages 5–17: U.S., 1998–2009,” available from the Health Data Interactive website. NHIS data were used to estimate ADHD prevalence for this HDI table.
NHIS data are collected continuously throughout the year for the Centers for Disease Control and Prevention’s (CDC) National Center for Health Statistics (NCHS) by interviewers from the U.S. Census Bureau. NHIS collects information about the health and health care of the civilian noninstitutionalized U.S. population. Interviews are conducted in respondents’ homes, but follow-ups to complete interviews may be conducted over the telephone. The Sample Child component collects detailed data on health conditions for a randomly selected child in households with at least one child. A responsible adult, usually a parent, responds to the survey questions as proxy for the sample child. For further information about NHIS and the questionnaire, visit the NHIS website.
NHIS is designed to yield a sample that is representative of the civilian noninstitutionalized population of the United States, and the survey uses weighting to produce national estimates. Data weighting procedures are described in more detail elsewhere (11). Point estimates and estimates of corresponding variances for the HDI estimates were calculated using SUDAAN software (12) to account for the complex sample design of NHIS. The Taylor series linearization method was chosen for variance estimation.
Differences between percentages were evaluated using two-sided significance tests at the 0.05 level. Terms such as “higher than” and “less than” indicate statistically significant differences. Terms such as “similar” and “no difference” indicate that the statistics being compared were not significantly different. Lack of comment regarding the difference between any two statistics does not necessarily suggest that the difference was tested and found to be not significant.
All estimates shown in this report have a relative standard error less than or equal to 30%. The significance of trends was tested using weighted least squares regression models of the log of each outcome and Joinpoint software (13) to determine whether an apparent change over time was statistically significant, taking into account the standard error for each data point.
Lara Akinbami, Xiang Liu, Patricia Pastor, and Cynthia Reuben are with the Centers for Disease Control and Prevention’s National Center for Health Statistics, Office of Analysis and Epidemiology.
Akinbami LJ, Liu X, Pastor PN, Reuben CA. Attention deficit hyperactivity disorder among children aged 5–17 years in the United States, 1998–2009. NCHS data brief, no 70. Hyattsville, MD: National Center for Health Statistics. 2011.
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
Edward J. Sondik, Ph.D., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Linda T. Bilheimer, Ph.D., Director
For related articles click:
ADHD Data and Statistics in The USA and ADHD Data & Statistics
To view HUNDREDS of articles and videos on ADD/ADHD, go to addrc.org
July 01, 2025 by addrcHarold Robert Meyer and The ADD Resource Center Why are people…
Why is it that even after we’ve made peace with someone’s actions, the memory lingers?…
Knowing that ADHD is manageable flips the script from despair to possibility. It’s not just…
If you care about your cognitive health or that of your children, understanding the impact…
As a teen with ADHD, you're navigating school, friendships, family expectations, and your own identity—all…
Harold Robert Meyer | The ADD Resource Center 06/21/2025 Executive Summary Speaking with authority can…
{kind=link}
{kind=link}
{kind=link}
{kind=link}